 UK Government Policy Turned Care Homes Into Death Camps
UK Government Policy Turned Care Homes Into Death Camps
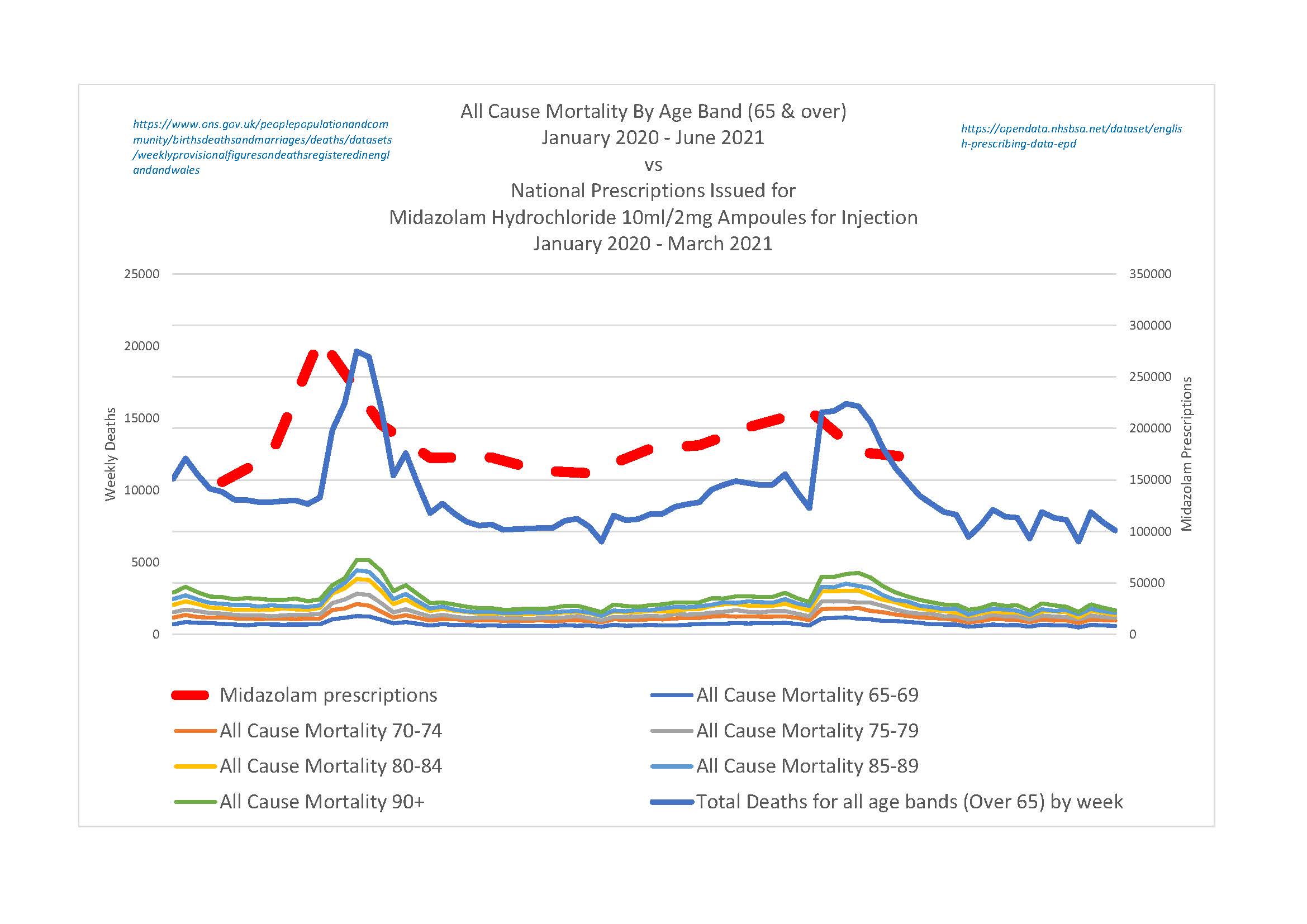
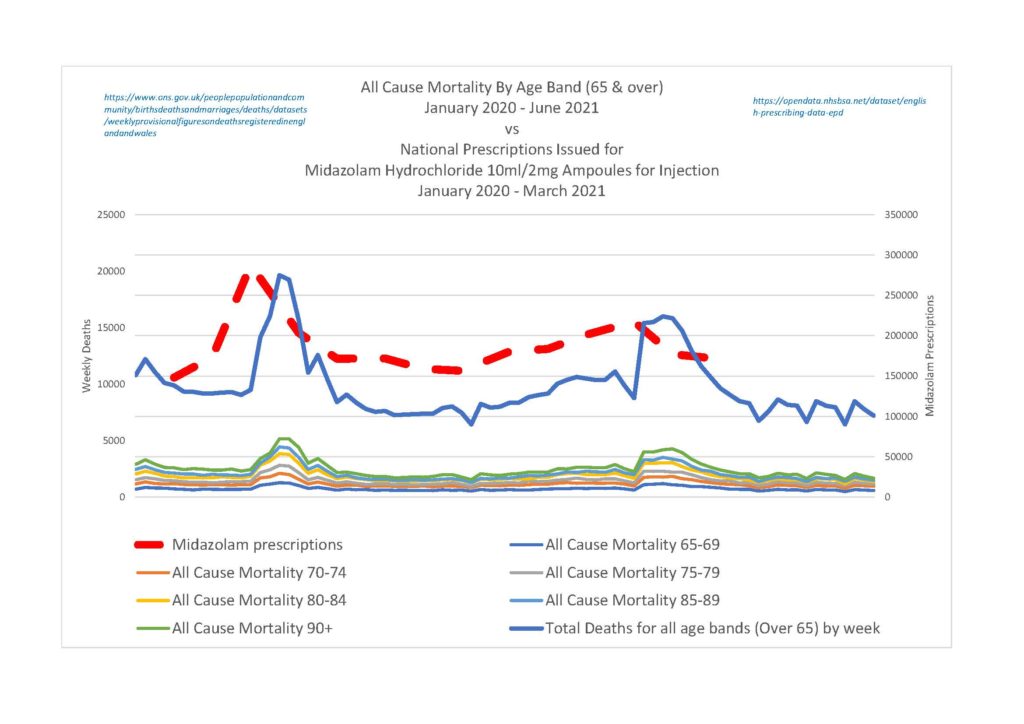
Over the course of the past eighteen months, it has become chillingly apparent to myself and the rest of the team who have been amassing prima facie evidence of genocidal fraud against the Four Horsemen and their accomplices that UK Government policy effectively turned Britain’s care homes into death camps, where the over 65’s, the sick and the disabled were dispatched with lethal doses of Midazolam and Morphine.
As the new updated criminal court papers entered the final stages of preparation, on Saturday morning we received a copy of a formerly confidential UK Government report written in July 2017, known as the Pandemic Influenza Briefing Paper.
This has transpired because of a successful FOI request for the information be made public, for the purposes of which, here lies a brief summary of the damning paper.
Suspension of Care
In section 4.4 of the UK Government’s briefing paper, the following were earmarked for prioritizing within the NHS, in the event of a ‘pandemic’, under the heading Primary Care Suspensions and Priorities:
Managing infections such as Sepsis, Cellulitis, Meningitis and Influenza.
Acute and urgent illnesses and trauma, such as fractures and acute abdominal pain.
Palliative, Pain Management and End of Life Care.
Conversely, in the list marked for suspension were:
All routine Dentistry and Optometry services.
Management of Chronic Disease.
Low level Mental Health Care [including treatment of patients with Learning Difficulties].
Routine Diabetes Screening.
Musculoskeletal Care.
Preventative Care [including ‘vaccination’, which is the only element of the plan which was not implemented in March 2020 by the UK Government, upon the advice of Hancock, Whitty, Vallance and Ferguson].
Dementia Diagnosis and Old Age / Frailty Management.
Decision Making
In section 5.0 on Decision Making, the briefing paper summarizes how the process of deciding when the suspension of the foregoing services and treatments would take place, as well as who would be denied them:
The Secretary of State for Health and other Ministers will be asked to decide that population triage can be enacted. This will allow NHS England to allow clinicians in local hospitals to make appropriate decisions about providing care to those patients who will benefit the most in a situation where the system is under extreme and unprecedented pressure.
The request for such a decision will be informed by insight from NHS England, NHS Improvement, the frontline and DH, as well as specialist advisory bodies established in response to a pandemic. Consideration will need to be taken as to whether such a decision is made at England level or nationally across all four UK countries.
Such a decision to move to population triage will effectively be an extension of the usual routine and daily clinical decisions made by clinicians regarding admissions and discharges. However, rather than decisions being made on a basis of triage by clinical outcome, triage by resource availability will also inform the decision.
From which we can easily glean that Matt Hancock [when he was still the secretary of state for the DHSC] and the government ministers in the Cabinet Office were asked to enact ‘Population Triage’ upon the advice of NHS England, NHS Improvement, civil servants within the DHSC and SAGE [which naturally included Neil Ferguson, Chris Whitty and Patrick Vallance].
Furthermore, the section also states that clinical decisions by clinicians on matters of admission and discharge would be based upon the treatment / service resources available, rather than ‘a basis of triage by clinical outcome’.
Ethics
Section 5.1 of the report states that the ethical framework underpinning the policies recommended was developed by the Committee on Ethical Aspects of Pandemic Influenza and published by the Department of Health in 2007 as guidance for dealing with ‘Pandemic Flu’, which in turn states that:
Equal concern and respect is the fundamental principle that underpins the ethical framework. This means that:
- everyone matters
- everyone matters equally – but this does not mean that everyone is treated the same
- the interests of each person are the concern of all of us, and of society
- the harm that might be suffered by every person matters, and so minimising the harm that a pandemic might cause is a central concern
The ethical framework section was developed by the Committee on Ethical Aspects of Pandemic Influenza and first published in 2007. It was revised by the Department of Health and Social Care in 2017.
In other words, whilst the framework insists that ‘everybody matters’, that ‘the harm suffered by every person matters’ and that ‘the harm that might be suffered by every person matters’, it also inserts the fatal caveat that this ‘does not mean that everyone is treated the same’.
Which is another way of saying that the harm suffered by some people [the over 65’s] is less important than the suffering endured by other people [the under 65’s]; which is akin to implicitly targeting a specific section of the population for elimination by denial of critical treatments and services.
Deactivation of Care & Expansion of ‘Good Deaths’
In a table called Activation and Deactivation of Primary and Secondary Care Activities, the briefing paper lays out the detailed plan for dealing with every aspect of every severity level of any kind of ‘pandemic’, in which it is stated that in the event of a moderate outbreak, End of Life Facilities should be supported and expanded, concurrent with the reduction of non-urgent services such as general, ENT and vascular surgery, as well as reducing cardiac and cancer surgery ‘as the situation develops’.
Furthermore, it is also recommended that, in the event the outbreak escalates to emergency level, the care patients receive should be determined by the resources available, rather than upon the health requirements in each individual case.
Mass Murder By Government Policy
All of which is starkly reminiscent of this three minute video, in which Dr Luke Evans MP introduces his questions for Hancock [in the House of Commons April 2020 inquiry into COVID-19] with the following statement:
“A Good Death requires three things…”
Those three things which Evans says every ‘Good Death’ requires are having enough syringes, enough Midazolam and Morphine and enough staff to administer the fatal doses of the drugs prescribed, within a supposedly ethical framework which repeatedly recommends scaling up End of Life Care, whilst denying critical care to the very people who were forced to sign Do Not Resuscitate notices before they were incapacitated with opiates and Midazolammed into premature death.
Nevertheless, it is immaterial whether they call it ‘A Good Death’ or not because what it all amounts to is yet more prima facie evidence of mass murder by UK Government policy, all of which substantiates the allegations in PUB’s Private Criminal Prosecution of the Four Horsemen and their accomplices.




